Polyvagal Theory bulletpoints
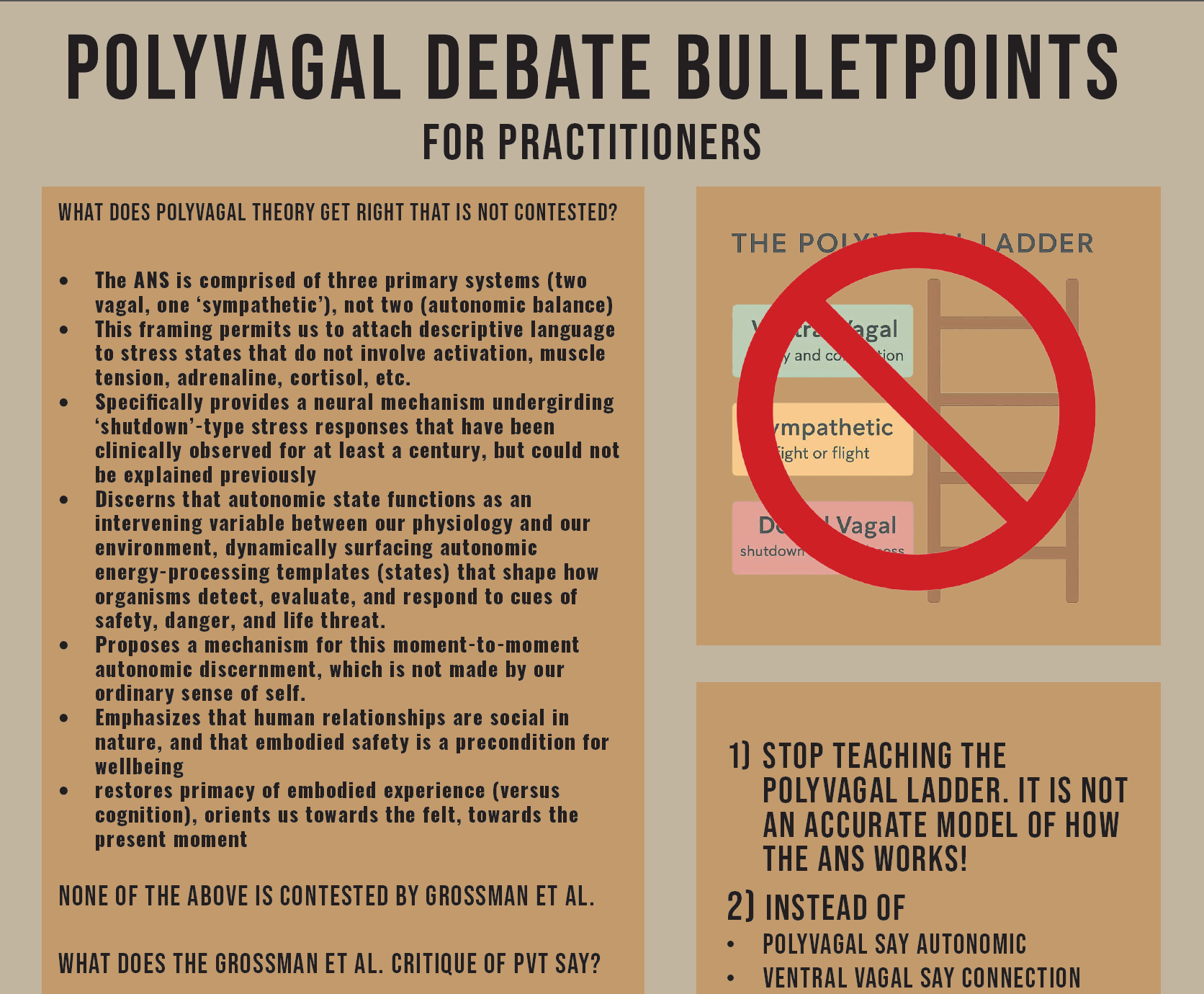
Bulletpoints for practitioners

This is not an official Polyvagal Institute perspective: I have no formal affiliation with Stephen W. Porges or PVI1 .
I am writing for people whose practical work involves supporting clients in felt moment-to-moment contact with the dynamism of the living nervous system, which would include therapists, bodyworkers, and coaches of all kinds. The people who have been putting Polyvagal Theory to practical, not theoretical use. The people who have witnessed its ability to help a person organize an understanding of how their bodymind is responding to the inner and outer world based on safety/danger and the historical accumulation of stress.
I am writing to help you discern signal from noise, smoke from fire in this debate, which is not advancing in the public spheres because both sides are dug in, for different reasons, one aggressive and one defensive, in ways that are understandable based on a variety of factors and yet ultimately not useful.
Let’s start with–
What does Polyvagal Theory get right at the level of theory
The ANS is comprised of three primary systems (two vagal, one ‘sympathetic2’), not two (autonomic balance)
This conceptual scaffolding permits us to attach descriptive language to stress states that do not involve activation, muscle tension, adrenaline, cortisol, etc.
Specifically providing a plausible neural mechanism undergirding ‘shutdown’-type stress responses that have been clinically observed for at least a century, but could not be explained previously
Autonomic state functions as an intervening variable between our physiology and our environment, surfacing neurophysiological platforms (energy-processing templates) that shape how organisms detect, evaluate, and respond to cues of safety, danger, and life threat.
Proposes a mechanism for this moment-to-moment autonomic discernment, which is not made by our ordinary sense of self. 3
So what and who cares? Why does this matter?
At a physiological level, PVT orients us towards
the importance of safety as an embodied experience shaping well and illbeing
awareness of the dynamism of the Autonomic Nervous System in responding to the moment-to-moment texture of our experience
the recognition that the same person in states of safety, danger, and lifethreat may be as different as liquid water, steam, and ice
At an ontological level (of being), PVT orients us towards embodiment, towards the notion that ‘I feel myself, and therefore I am.’
This is a corrective to a Cartesian worldview that locates identity in thinking
It restores primacy to embodied experience, to the felt, to the present moment
At a phenomenological level, PVT orients us to the direct experience of the embodied nervous system, rather than the story we tell ourselves about what happened
What did you notice, rather than what did you think
this expands the tactical surface area of intervention available for transforming our experiences to include sensation, images, tactile experience, behavior, perception, affect, and meaning which substantively broadens the range of interventions we might bring to bear to support someone
At an epistemological level (how do we know what we know), PVT orients us to meaning-making in the felt relational fabric between people, and in particular to moment-to-moment awareness of our sense of sufficient embodied safety as a precondition for healthy relating
At the level of lineage history (deep human ancestral understanding) PVT aligns with a view that Small Band Hunter Gatherers are the baseline of human normalcy, and that safety and connection are species-normal attributes
This is a corrective to prevailing notions that ‘life in a state of nature is solitary, poor, nasty, brutish, and short’ (Thomas Hobbes, 1651, Leviathan)
It reminds us that human wellbeing is social in nature, and that part of the role of ‘society’ is to reinforce this social nature, not undermine it
At a public health level, PVT orients us to attend to safety as a public health need: a precondition for thriving, not a privilege but a human right
Importantly, none of the above is at issue in the Grossman critique. Most of the above is entirely outside the sphere of what Grossman and colleagues are critiquing. You can continue to assert any and all of the above without saying anything controversial in the least.
What does the Grossman et al. critique of PVT say:
Respiratory Sinus Arrhythmia is not a direct and reliable measure of central vagal outflow to the heart. This is asserted to be a methodological error in PVT.
PVT characterizations regarding the neuroanatomy and functions of two major brainstem vagal nucleii (the ventrally situated Nucleus Ambiguus and the Dorsal Motor Nucleus of the vagus nerve) are not accurate
PVT assertions regarding the evolution of the vagus nerve are not accurate
PVT claims about the specificity of mammalian social behavior in relation to nonmammalian vertebrates are not accurate, and
PVT interpretations of earlier seminal physiological literature are not accurate.
So what and who cares? What is at issue and why does it matter?
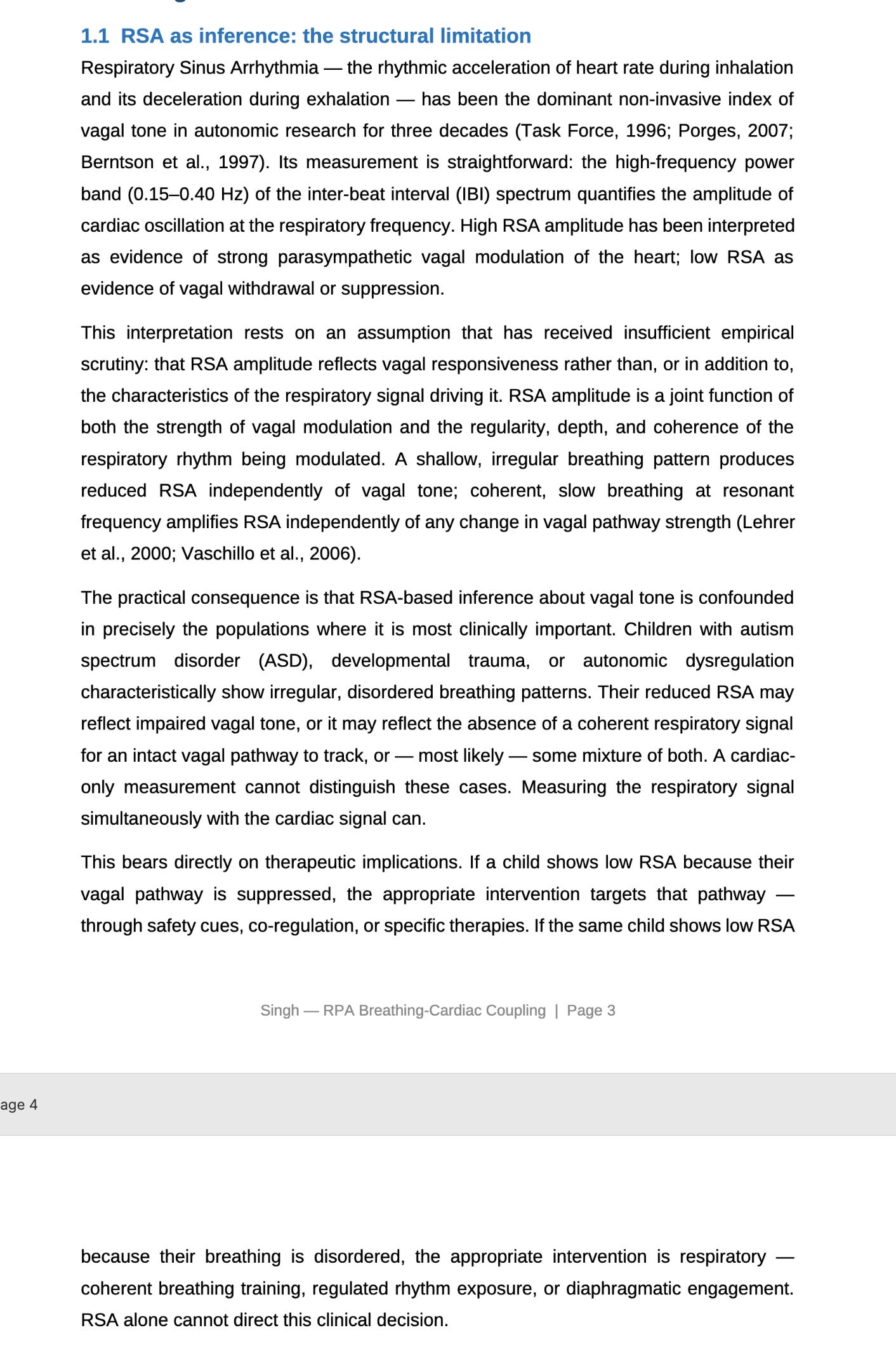
The primary autonomic signal that Stephen W. Porges, PhD used to measure/ organize vagal tone is a cardiac signal called Respiratory Sinus Arrhythmia. “Respiratory Sinus Arrhythmia — the rhythmic acceleration of heart rate during inhalation and its deceleration during exhalation — has been the dominant non-invasive index of vagal tone in autonomic research for three decades (Task Force, 1996; Porges, 2007;Berntson et al., 1997).”4 Grossman is saying that this signal is not a reliable metric of central vagal outflow to the heart (because it is coupled with other systems and feedback loops).5 This is true. RSA is not, in fact, the optimal or primary autonomic signal in the body. This is an accurate methodological limitation – RSA cannot separate respiratory drive from vagal responsiveness, and this is true whether or not PVT’s specific anatomical claims are correct. What is to be done? Porges and colleagues (or someone else, as they don’t seem inclinced to do this) should evaluate the claims of PVT using alternative autonomic diagnostic metrics. WE RECOMMEND USING RESPIRATION.
Until an alternative set of autonomic diagnostic metrics confirms PVT assertions, Grossman’s assertion that RSA is problematic is sustained.
The discussion about brainstem vagal nucleii, the evolution of the vagus nerve, and the specificity of mammalian social behavior all directly bears on PVT assertions about the autonomic ladder, and a hierarchy of autonomic state. Porges himself has stated that the evolutionary claims are speculative. You can hear him say this, verbatim, right here in my 2021 interview with him (see 8 minutes 30 seconds or so). This is really the meat of the rebuttal to PVT. Grossman is saying that experimental studies of the vagus nerve, the ANS in vertebrates, and established phylogenetic inferences of social evolution in vertebrates contradict the assertions of PVT.6 What I would like to direct your attention to in the Grossman critique is the phrase ‘established phylogenetic inferences of social evolution in vertebrates.’ What is an inference? A conclusion based on evidence and reasoning. An inference is not a fact. It is not a law. It is not an axiom. In the parlance of science, an inference is a best guess. So in plain language, Grossman is saying that the collective best guess of the leading vagal physiologists about the differentiation between the vagal brainstem nucleii, evolution of the vagus, and specificity of mammalian social behavior contradicts the best guess of Stephen W. Porges, PhD.
To err on the side of caution, this suggests that equating the Dorsal Motor Nucleus (DMX) with shutdown MAY be tenuous. It suggests that equating the Nucleus Ambiguus with social engagement MAY be tenuous. Or, the established inferences may be wrong. Or (what I think), Porges has got it partly right, and the established field has it partly right, and neither have it fully right.
What is a theory anyway?
A theory is an explanatory scaffold. Theories in science endure to the extent that they can explain observed phenomena. We thought the earth was at the center of the solar system (the cosmos in fact) for most of human history. At a certain point– not that long ago– there were enough phenomena that could not be explained by this geocentric theory that it collapsed. The field entered a period of disruptive upheaval, and eventually a heliocentric model (sun as center of the solar system) came to bear. This model better explained observable phenomena (retrograde motion of the planets, for example) than the previous earth-centered model.
The evolutionary claims of both PVT and a consensus of vagal anatomists are relatively difficult to adjudicate, because the phenomena they are describing changed several hundred million years ago. We can argue in an impassioned way about whether or not this brainstem nucleii migrated ventrally, but such arguments will always be inferred, because no one alive now witnessed this taking place. Not Porges, not Grossman, not any of the 38 signatories to the Grossman paper.
What PVT brings to bear is a plausible explanatory mechanism. What Grossman’s critique does, usefully, is assert that this mechanism is speculative, and at odds with the general understanding of the field. I happen to agree with Grossman specifically about the fact that the brainstem nucleii theory of PVT is not accurate, but not for the same reasons Grossman disagrees. Because– take a deep breath– the entire field of vagal physiologists could also be wrong. Because - get this- evidence of the DMX’s failure to elicit bradycardia (sudden drop in heart-rate) may not mean it doesn’t. It just might not do this unless there is the neuroception of lifethreat, release of endogenous opioids, and apnea– none of which have ever been tested in a research setting. Because- and PVT is flat wrong about this– the subdiaphgramatic vagus has a role in health creation as well as in lifethreat responses. Yet here’s the thing– I don’t actually think that these claims will be definitively adjudicated one way or another as currently constructed. And I’m not sure it matters. Why doesn’t it matter?
Because Polyvagal Theory already cannot explain a great number of phenomena that we don’t have to speculate about things that happened 200 million years to notice.
What can PVT not explain that we don’t have to speculate about 200 million years of vertebrate evolution to notice?
PVT cannot explain
Why does a certain percentage of the clinical population shift out of shutdown responses and directly back into autonomic connection/ social engagement states without moving through sympathetic states? If autonomic state is a ladder, with social at the top, and dorsal at the bottom, a person moving out of dorsal would have to move through sympathetic to come to social. While this happens in our clinical experience about 80% of the time, we have observed a statistically significant percentage of the population that moves out of shutdown back into connection. This is direct experiential clinical confirmation that the ANS is not a ladder. If it were a ladder, you could not skip from ‘dorsal’ to ‘ventral/social’ without passing through sympathetic.
If the DMX is uniquely associated with shutdown responses, and regulates the enteric nervous system (sub-diapghragmatic autonomic/ vagal architecture) how come there is rhythmic coordination in newborns between the suck/swallow reflex (proposed to be ventral vagally mediated by the NA in PVT) and pulsation of the anus (proposed to be mediated by the DMX in PVT)? Answer? Because the ventral and dorsal vagus coordinate in health-creating states. PVT does not understand this.
How/why do certain shutdown phenomena localize in body parts other than the sub-diaphragmatic vagus? If the unmyelinated vagus under the respiratory diaphragm is the neural architecture of shutdown responses, why do we observe in clinic that people regularly experience ‘localized shutdown’ in a shoulder, knee, one side of the body, other joint, etc.?
How do we explain states that are ‘sympathetic’ that have no activation (adrenaline/cortisol)? States of play make use of the ‘sympathetic’ movement architecture, but do not contain activation chemistry.7
I could go on…
What do you need to do differently in your practice to be responsible to this moment of debate and challenge to PVT
stop talking about the ‘autonomic ladder’ and using diagrams like this. This is not how your Autonomic Nervous System works. If it were truly this simple, anyone on TikTok or Instagram could go around claiming they were a nervous system expert. Oh wait…:
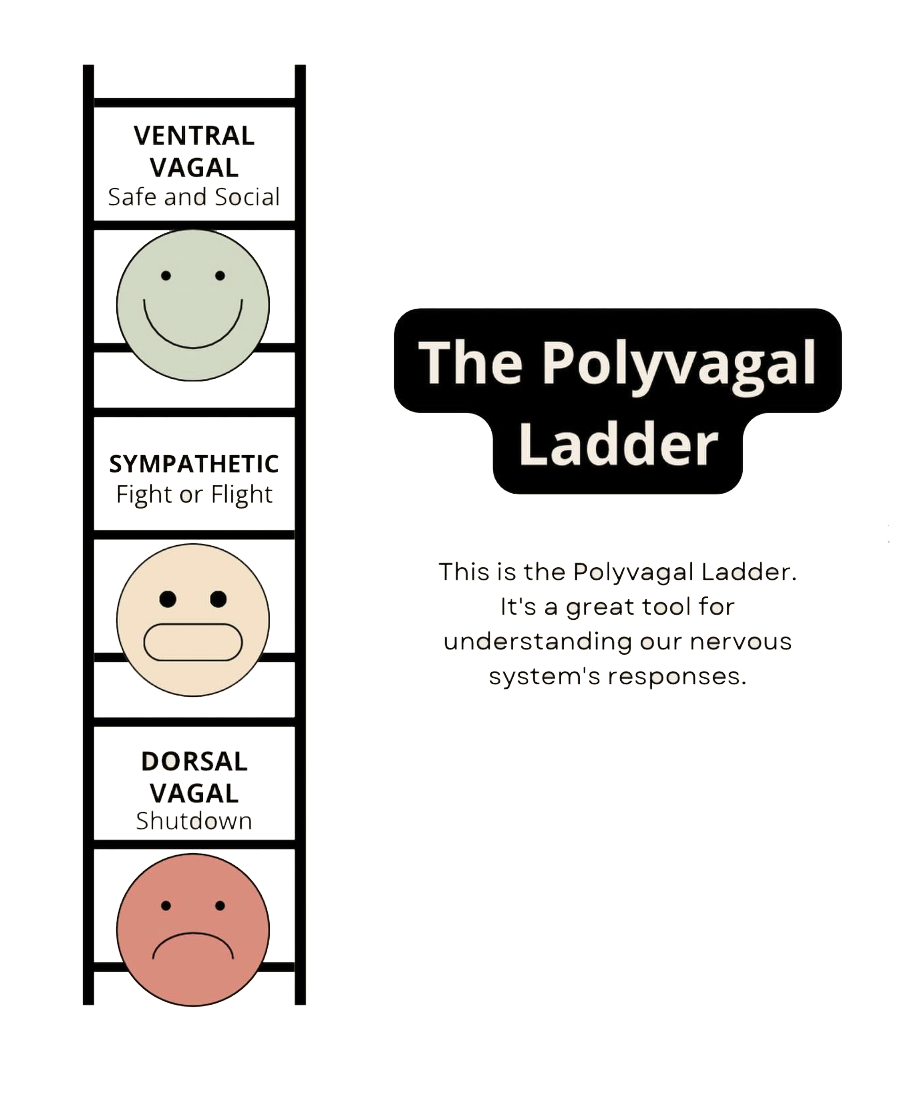
Instead of saying ‘your ventral vagal system’ say ‘your CONNECTION system’. If you are talking about lifethreat and shutdown, instead of ‘dorsal vagal complex’ say SHUTDOWN response. In other words, describe the ACTION OF THE AUTONOMIC NERVOUS SYSTEM, not the ‘brainstem source nucleii’ that have not been conclusively tied to them.
Don’t teach your clients things that you don’t understand. I’ve heard so many practitioners saying - Well, I never REALLY understood PVT. Why on earth are you teaching people something you do not understand? That is not ethical. Stop doing that.
Do your research. Discern which sources of information are viable. Engage primary sources. I encourage you to read the research papers. Grossman’s paper is here. Porges’ rebuttal is here.
Polyvagal Theory has been operationalized both through Polyvagal Institute courses, and through two listening therapies patented by Stephen Porges’ company Polyvagal Science LLC, and licensed by the Canadian neurotechnology company Unyte. They have released the Safe and Sound Protocol (SSP), and the Rest and Restore Protocol (RRP). There are numerous reports of the SSP engendering adverse reactions in clients. Unyte was actually warned about this by their original Clinical Advisory Board prior to the release of the product, and proceeded to fire the Advisory board. There are at least three reasons that the SSP might cause problems
It is administered to someone who is not a good candidate for it
the dose administered is not properly sized
the practitioner administering it is not properly trained
All the above duly noted, there are also clients for whom the SSP is an extraordinarily supportive intervention. The RRP is an extraordinarily supportive intervention. The fact that these tools work at all is evidence that PVT is not categorically false. If you are using these tools, use them responsibly and understand their limitations and contra-indications.
What actions might you take to feel like you are doing something proactive about this?
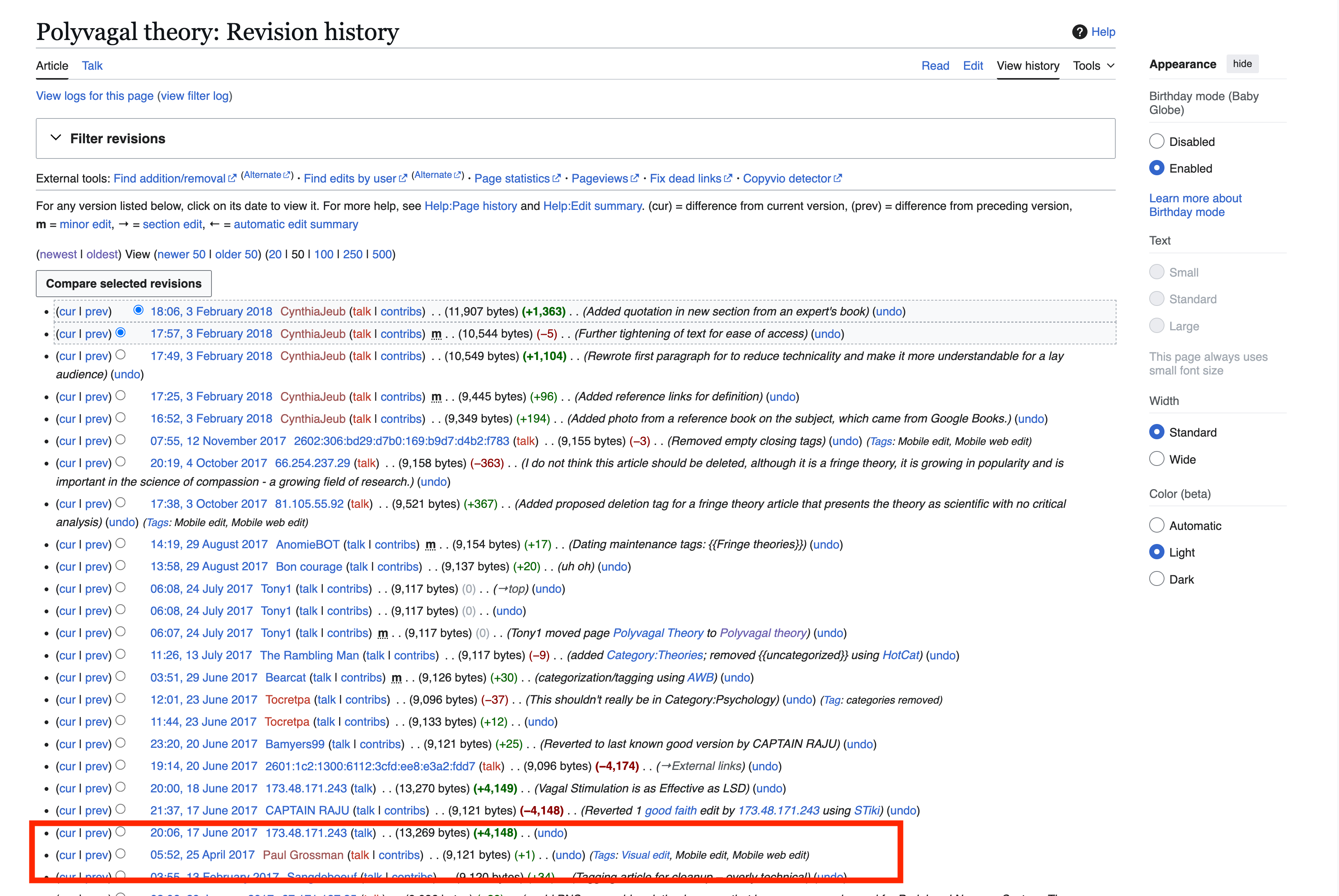
If you have found Polyvagal Theory important to your understanding of the work that you do, encourage Stephen W. Porges, PhD and the Polyvagal Institute to substantively engage the critique. I get it– Grossman is angry, aggressive, disingenuous, and obstreperous. He is seeking a takedown. This seems like a vendetta. He has been publicly tampering with the PVT Wikipedia page for years. (He lost his mind when I asserted this publicly, but the editing record is transparent. If you’d like to see his edit history, go to Polyvagal Theory’s Wikipedia page, and visit the revision history. Go back to 2017. Look for an editor named ‘Paul Grossman’.8 Since around that time algorithmic editing of the page has pushed it in the direction of fringe science, and all changes that have sought to bring neutrality to the page have been overwritten, largely by the algorithmic censor MrOllie.) But as problematic a person as Grossman is, categorically asserting that he is attacking a straw man of the theory and that this has already been responded to amounts, functionally, to the Developers and stewards of Polyvagal Theory exhibiting a shutdown response in relationship to being challenged. Rather, encourage them to do the more difficult work of engaging the critique. Attempt to validate PVT through a different autonomic diagnostic than RSA, for example the Respiratory Profiling Analysis tool developed by Samar Singh, PhD.
Resources
Our one page PDF entitled ‘Polyvagal Bulletpoints for Practitioners’ is free and shared under creative commons attribution. Downloading it will put you on our mailing list (stated for transparency), from which you can opt-out if you wish.
My new book, Autonomics: Placing the Lineage History of Neuroscience on a Sacred Foundation, deeply explores not just our history with the Polyvagal Theory (I have been quite involved with Porges and the Polyvagal community historically) but how the orthodox mechanisms for assembling ‘validated’ medical knowledge fundamentally deny the reality of the lineage history of scientific breakthrough in the disciplines. You can read the preface to the book at the purchase link.
Hearth Science teaches autonomic physiology to wellness professionals internationally, as well as interested laypeople. You can see all of our classes, as well as their level of difficulty (when working with wellness professionals we assume a basic knowledge of neurology), when working with the general population we assume no relevant scientific background, here.
I did however write and art direct the Official Polyvagal Posters (2020) and my firm did have an intellectual property development agreement with Polyvagal Science, LLC. I did write this article in Psychology Today about Polyvagal Theory through the lens of water. I did interview Stephen W. Porges, PhD on multiple occasions. I also ran the Polyvagal Study group on Facebook, which contained about 5,000 wellness professionals studying Polyvagal Theory around the world, and I left because our own work at the translation research firm I direct was gathering clinical data that contradicted Polyvagal Theory. I did also take a phone call with the Executive Director of the Polyvagal Institute, when this whole debate started, who asked for my advice. So far they have not acted on what I advised them, which was in part to publish a list of the professional collaborators, colleagues, and allies with whom Stephen W. Porges, PhD has, and continues to collaborate, to undermine the false narrative that Paul Grossman’s position is affirmed by 38 of the world’s leading experts on the Vagus, and Porges is a ‘lonely pyschologist’. This is simply not true, and never was.
This is already problematic, because the notion of a ‘Sympathetic’ Nervous System reflects an antique understanding of both the neurology and the neurochemisty of the vertebrate Movement System. Tacking this mis-naming is beyond the immediate scope and utility of this commentary, yet is none the less necessary ultimately if we are to advance this discourse
Whether the neurophysiological mechanism of this is understood or not is a secondary consideration. PVT calls this ‘neuroception’. We call it ‘autonomic temperature’. Your ordinary egoic sense of self is not the phenomenon making this assessment.
(PDF) Measuring the Conductor and the Orchestra. Available from: https://www.researchgate.net/publication/401680678_Measuring_the_Conductor_and_the_Orchestra
https://www.researchgate.net/publication/401680678_Measuring_the_Conductor_and_the_Orchestra
A relevant excerpt from the paper (MacDuffie & Singh, 2026) is below:
This is directly from the Grossman paper: “We base our arguments upon experimental studies of the vagus nerve and the autonomic nervous system in vertebrates carried out for the past six decades, and on well-established phylogenetic inferences of social evolution in vertebrates.” (from https://www.clinicalneuropsychiatry.org/download/why-the-polyvagal-theory-is-untenable-an-international-expert-evaluation-of-the-polyvagal-theory-and-commentary-upon-porges-s-w-2025-polyvagal-theory-current-status-clinical-applications-and/)
PVT cannot explain this, but neither can traditional neuroscience. (Dee Wagner, The Developer of Chi for Two® first brought this awareness to our attention in the Polyvagal Study group.)
Polyvagal Theory Wikipedia editing history excerpt: