

An Autonomics Framework for updating Polyvagal Theory to render the Grossman critique largely irrelevant

@HeatherMacduffiePhD, @SamarSinghPhd, @karenonderkdo, @drjeffrockwell, @anadovalleOTR, @kimbarthels, @UNYTE, @PVI, @PolyvgalTheory, @StephenPorgesPhD, @RobertNaviauxMD, @EricGordonMD, @JDDanielsMD, Bruce Cryer Marcia Miller Darcia Narvaez Four ARROWS @debdanaLCSW Randall Redfield

Let’s first be clear about whom this update is intended for. It is not Grossman, because the gentleman has made it abundantly clear that he is interested in a takedown, not the evolution of the theory. It is also not for the myriad individuals piling on to the Grossman critique for various reasons, including that controversy generates clicks, that people like to see a good fight, pundits are gonna pundit, etc.
My Linkedin feed has been filled with this kind of garbage for the past week, since Grossman published his WHY THE POLYVAGAL THEORY IS UNTENABLE ‘refutation’. (That is a journal article in the peer-review journal Clinical Neuropsychiatry, and yes, the title is in ALL CAPS.) Let’s be clear: Grossman has been the antagonist of this work for decades: he has finally organized a ‘reputable’ assembly of colleagues to back him up (38 of them).
Grossman’s paper is not wrong. Grossman’s neuro-anatomical and measurement critiques hold water, but they throw the baby out with the bathwater, which is what he has been trying to do all along.
Numerous parties, including Grossman, continue to label the theory as pseudo-science, myth, etc. Polyvagal Theory is neither myth nor pseudo-science: it is a trans-disciplinary synthesis. Stephen W. Porges, PhD, has, in his career, published more than 400 peer-review articles in the literature. He is Distinguished University Scientist at Indiana University where he is the founding director of the Traumatic Stress Research Consortium. He is Professor of Psychiatry at the University of North Carolina, and Professor Emeritus at both the University of Illinois at Chicago and the University of Maryland. Pseudo-scientists do not have 400 peer-review publications. Pseudo-scientists do not have three university professorships and a distinguished scientist appointment. Pseudo-scientists generally do not patent psychophysiology methods and systems.
Grossman has also continually actively tampered with Stephen Porges’ public internet presence, repeatedly altering the Wikipedia pages for both his personal bio, and Polyvagal Theory. The Polyvagal Institute has attempted to work with Wikipedia on this (anyone can edit anything on their site, more or less), has engaged consultants, and sought legal counsel. Porges himself simply refuses to engage at this level, yet unfortunately Grossman has succeeded in damaging the discourse around the theory because ostensibly neutral representations of the work are now negatively biased because they were tampered with. I know this because I spoke with the Executive Director of the Polyvagal Institute about putting together a team to over-write the continual updates Grossman was making to their Wikipedia page. He told me they would address this; they have not yet succeeded. Unfortunately, the internet is the doorway to adjudicating this in the court of public opinion, where it is being decided by people with the least likelihood of understanding the nuances involved, and where the people who SHOUT THE LOUDEST are drowning out calmer and demonstrably more informed voices.
Because Grossman’s agenda is not to identify the elements in Polyvagal Theory that can be further refined in service to a more comprehensive understanding of in vivo autonomic physiology, he has consistently refused to respond within the context of Porges’ methodological request.
In Porges’ words, from the same issue of Clinical Neuropsychiatry:
A recent critique advanced by Grossman et al. (2026, this issue) argues that Polyvagal Theory is scientifically untenable, asserting that its core claims regarding autonomic organization, respiratory sinus arrhythmia (RSA), and evolutionary framing are inconsistent with established neurophysiology. The present paper evaluates these assertions not by disputing individual claims in isolation, but by examining whether the critique engages Polyvagal Theory as it is articulated in the peer-reviewed literature and whether it meets the epistemic standards required for scientific refutation.
Rather than responding sequentially to individual objections, the analysis clarifies the theory’s conceptual foundations, scope, and explicit conditions of falsifiability as a systems-level, pathway-specific framework of autonomic state regulation. It demonstrates that the critique repeatedly evaluates a reconstructed proxy of the theory shaped by persistent category errors, including conflation of neuroanatomy with neurophysiology, reduction of theory to measurement, and substitution of phylogenetic continuity for functional organization. These structural misrepresentations propagate across methodological, neurophysiological, evolutionary, and developmental domains, precluding meaningful empirical adjudication.
Across these domains, the paper shows that disagreements concerning RSA metrics, comparative anatomy, or evolutionary framing do not engage the theory’s specified mechanisms or demonstrate conditions under which its predictions would fail. Where disagreement exists, it reflects differences in measurement preference, level of analysis, or theoretical framing rather than evidence against the theory’s organizing principles. An appendix presents a historical audit showing that several central claims reiterated in the critique were identified in the literature nearly two decades earlier as mischaracterizations of Polyvagal Theory. Their continued repetition without substantive modification reflects a persistent failure of representational uptake rather than unresolved empirical controversy.
It is concluded that the charge of scientific untenability does not apply to Polyvagal Theory as formulated, but instead reflects a critique that fails to engage the theory on its own terms. Productive scientific discourse requires representational fidelity, appropriate alignment of levels of analysis, and responsiveness to theoretical and empirical clarification ‒ criteria essential to theory evaluation but not met in the critique under review.1

I would like, therefore, in the service of productive scientific discourse, and with representational fidelity to the Polyvagal Theory, to present a series of pathways for PVT’s substantive neurophysiological revisioning into a form that renders the Grossman critique largely irrelevant. I would be happy to meet with Stephen W. Porges, PhD at any time to discuss this. You and your team have my contact information, Sir.
By way of full disclosure, I am the Founder of the translation research firm Hearth Science, in which capacity I have, for the past 15 years, been leading a trans-disciplinary research collective studying the living autonomic nervous system. I collaborated with Porges from 2019-2021. My firm had an active intellectual property co-development agreement with Polyvagal Science, LLC until 2024. I wrote and art directed the Official Polyvagal Theory posters under Steve’s guidance (reviewed by Deb Dana, LCSW). For a number of years I contributed to, and then ran the global Polyvagal Study Group on Facebook, a group of about 5,000 wellness professionals around the world studying Polyvagal Theory. I was asked to lead the group due to the innovations my trans-disciplinary research firm was making in understanding the theory. I was subsequently invited to leave the group when these innovations crossed a line of ‘orthodoxy’ and were no longer considered to be ‘Polyvagal’ so I am well familiar with the discourse parameters established by the Polyvagal community regarding what constitute the acceptable foundations of the theory.
Stephen Porges has said, since 1994, that Polyvagal Theory could be proved wrong. He is aware that the theory is incomplete.
SO, WHAT HAS POLYVAGAL THEORY GOTTEN RIGHT (IN MY HUMBLE OPINION) AND AS IMPORTANTLY, WHY DOES IT MATTER?
Three Autonomic Systems
Stephen Porges’ recognition that the 10th cranial nerve, the Vagus, is not a single nerve, but rather a conduit that holds multiple vagal systems (one supra-diaphragmatic, one sub-diaphragmatic), subtending distinct visceral systems, with distinct physiological pathways, and differentially involved in responses to safety, danger, and lifethreat is THE MAJOR AUTONOMIC DISCOVERY of the second half of the 20th century, and for which Porges should receive the Nobel Prize in Physiology or Medicine. It is that important.
This updates the still-taught-in-medical-school-though-it-is-a-hundred-years-out-of-date notion of autonomic balance between the ‘parasympathetic’ and ‘sympathetic’ branches of the ANS. Autonomic balance is demonstrably false, yet almost everyone in the world who knows anything about the ANS as a mediator of stress responses believes that this is how it works.
The cultural import of this profoundly antiquated understanding cannot be over-stated. Autonomic balance is built into medical models, and underpins the algorithms running the HRV sensors in your smart watch, which is why their algorithms are not accurate.
Interoception as ontological
Porges orients us towards interoceptive awareness as a metric of being. He suggests that rather than an identity resident in thinking, interoception is the location of our experience of embodied self, and where we might find ourselves at home.
It is not, as Descartes would have it, I think therefore I am. It is I feel (myself), therefore I am.
This is a fundamental re-orientation of being from cognition to embodied (interoceptive) awareness.
This is a fundamental cultural fulcrum; an antidote to much of what ails modernity.
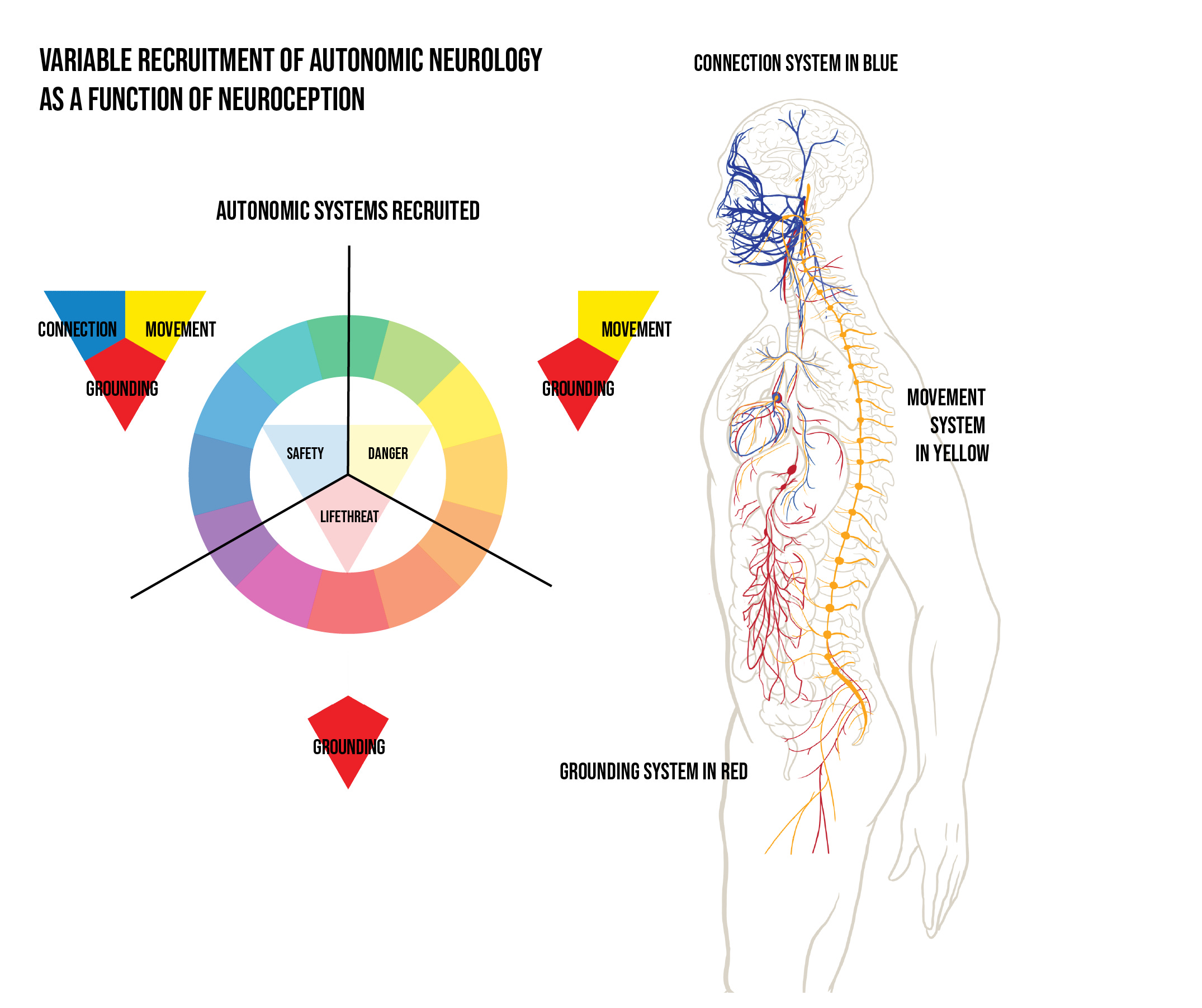
Variable recruitment of autonomic systems across the range of safety, danger, and lifethreat
Porges proposes a neurological mechanism (he coined the term neuroception) for the body’s moment-to-moment detection of safety, danger, or lifethreat.
Depending on whether the body feels safe enough to become available relationally (social engagement) or rather moves into states of defense (fight-flight, shutdown, etc.) the three autonomic systems engage differentially.
The three autonomic neurologies are differentially available depending on whether someone is experiencing safety, danger, or lifethreat.
This is easily verifiable, and correct.
This matters broadly because people’s autonomic nervous system is recalibrating moment-to-moment based on whether we feel safe, in danger, or under lifethreat. For most people, this is happening entirely outside of conscious awareness. If people understood this, and had interoceptive access to what it means, we would live very different (and better) lives.
Safety is a pre-condition of sociality, which is a precondition for wellbeing.
Inadequate access to safety is a public health issue, possibly the public health issue of our time.
We talk about disparities in access to housing, food, money, etc., but our public health discourse does not penetrate to the strata beneath this, which is the inequitable distribution of safety.
When people feel safe enough in their bodies, they have access to different visceral states, emotions, cognitions, perceptions of the world around them, and different behaviors. They develop a different existential sense of self. The foundational substate of this experience is physiological, not psychological.
For the past 12,000 years, humans have been moving away from our species normal ancestral baseline in safety and connection, into normalized states of physiological defense. The entire edifice of modern civilization, and therefore the polycrisis of modernity, is the neurobiological sequelae of humans who have moved into chronic states of defense. Our modern concepts of economy, nation state, politics, family, business organization are derivative of a normalization of modes of defense being conflated with modes of being.
We are therefore generating culture and civilization from the perspective of traumatized and neurobiologically dysfunctional humans, who have been acculturated to think this is species normal. It is not. We call these things human nature, but they are the products of a traumatized human nature: people whose bodies are accustomed to operating in response to chronic danger and do not know this. This is what makes policies and politics of division and threat so insidiously dangerous to our humanness.
We need safety to come home to ourselves. Polyvagal Theory taught the world this in the language of neurophysiology.
Human wellbeing is social in nature
The evolutionary species’ normal of the human lineage is the small band hunter gatherer group. Human wellbeing is social in nature. What Porges calls the ‘ventral vagal’ system (supra-diaphragmatic vagus), which undergirds the ‘social engagement complex’ that unites the neural regulation of the face, voice, tuning of the middle ear, turning of the neck and head, with the heart and the lungs, is the neurophysiological system whose availability is required as the prelude to secure attachment.
The discovery of this complex is an extraordinary piece of neurological detective work. Steve intuited this partly from his own experience playing clarinet, and partly from the ‘vagal paradox’, and discovered plausible evolutionary mechanisms for the differentiation of this circuitry in forward migration of neurons in the NA from the DMX. The veracity of these assertions, based on comparive evolutionary neuro-anatomy is beyond my scope, but the existence of the social engagement complex is demonstrably correct and easily verifiable.
The PVT neuro-anatomical description of this system is, however, beyond infancy, incomplete.
That this system needs to engage in a newborn for the baby to successfully co-regulate with a caregiver and successfully coordinate interoceptive visceral functions is, again, easily verifiable, and correct.
States of chronic defense are incompatible with wellbeing and become a primary substrate for illbeing
The movement into chronic states of defense, which decouples the ventral vagal system from the other two autonomic systems, prevents the body from coordinating states of health, growth, and restoration.
Sustained shifts into defense provide a primary physiological substrate of most classes of illbeing. (80% of what brings people into primary care is stress-related: this is the mechanism.)
When autonomic physiology is centralized as the diagnostic access of disease etiology, it transforms our understanding of the mechanisms of much disease.
This reorientation of disease taxonomy is inspired by Polyvagal Theory.

In summary, for advancing the field of autonomic physiology, and its application to the development of clinical and therapeutic models and neurotechnologies that demonstrably enhance human flourishing and illuminate the causes of suffering, Stephen W. Porges, PhD, should be accorded the highest honors bestowable on a scientist for work that benefits all of humanity.
His work is the most important work done in the autonomic physiology in the second half of the 20th century.
WHAT HAS POLYVAGAL THEORY MISSED (AND AS IMPORTANTLY, WHY).
THERE ARE TWO PRIMARY CATEGORIES OF ERROR IN PVT. SOME OF THEM ARE IN THE CONCEPTUALIZATION OF THE THEORY ITSELF. SOME OF THEM ARE IN THE FOUNDATIONS OF NEUROSCIENCE, AND THEREFORE PERMEATE THE FIELD AND CORRUPTED FOUNDATION ASSUMPTIONS THAT FED INTO PVT. I WILL ADDRESS THEM SEPARATELY.
FIRST, ERRORS IN THE POLYVAGAL CONCEPTUALIZATION.
RSA is not the most complete autonomic signal
The first part of the Grossman critique (I wrote about this yesterday here) is that Respiratory sinus arrhythmia is not a direct and reliable measure of central vagal outflow to the heart (mediated by the ventrally located brainstem Nucleus Ambiguus)
This is true. Its implications also extend far beyond Polvyagal Theory. If RSA is not a direct and reliable measure of central vagal outflow, every heart-rate variability monitor in the world is wrong, including the one you are wearing on your wrist. Your wearables are wrong. Your health-tracking ring is wrong, et cetera.
I’ve written about this extensively here, in this white paper: AUTONOMIC DIAGNOSTICS: Towards Accurate In Vivo Autonomic Measurement
From the paper: Although HRV (Heartrate Variability) metrics have become the de facto standard for autonomic measurement, this is not due to the intrinsic superiority of HRV as an autonomic signal, but rather largely due to historical factors related to its measurability and the available compute in the 1960s when psychophysiology techniques were initially developed and deployed to measure autonomic phenomena in vivo. Respiration is a more complete autonomic signal…
I would propose that Stephen Porges would have developed a very different articulation of Polyvagal Theory had he been looking at the realtime functioning of the ANS through the lens of respiration, rather than cardiac control.
Solution: PVT should be validated using a different autonomic measurement tool.
Recommendation: Use respiration as primary signal, not RSA/ HRV.
The Autonomic Nervous System is not a ladder
I have been writing about this for years. It is part of what got me uninvited to lead the Polyvagal Study group. Despite the fact that Polvyagal Institute teaches the ANS as a hierarchy, with ventral at the top, and dorsal at the bottom, and frames this understanding by way of reference to Jacksonian Dissolution, which is the notion that in dealing with a threat we recruit the evolutionarily newest autonomic systems until they fail, and then fall back to the next oldest systems, this is not how the ANS constructs autonomic state. Were only we this simple!
Polyvagal Conceptualization of state is inadequate
The Polvyagal conceptualization of autonomic state, its notion of which autonomic states exist, and their conceptual arrangement is not accurate or complete. Humans routinely flow in and out of autonomic states that are not on the Polyvagal map, and the composition of health-creating states is not correct. The notion of hybrid states is incomplete. The ‘sympathetic’ nervous system is regularly recruited without danger. Variable neurochemstries of connection, activation, and shutdown create polyphonic modes of autonomic states with degrees of nuance. The subdiaphragmatic vagus (PVT - dorsal vagus) is actually recruited in states where we have the neuroception of safety.
[The Polyvagal arguments about functional differentiation between NA/ DMX are speculative, and refuted directly by Grossman here:
GROSSMAN: Specious functional distinctions between vagal dorsal (Dorsal Motor Nucleus) and ventral (Nucleus Ambiguus) regions of the brainstem
Primary to PVT is the idea that human behavioral functioning to aversive and appetitive psychosocial stimuli depends upon a hierarchy of autonomic responses: First, calm and prosocial behavior is said to be parasympathetically mediated by the brainstem “ventral vagal complex” (most directly, the Nucleus Ambiguus [NA]). Second, PVT asserts that individuals experiencing severe stress mount sympathetic nervous system reactions of fight or flight. Third, in very dire or life-threatening circumstance, a defensive pattern of emotional freezing or psychological dissociation may occur, which is parasympathetically mediated by the Dorsal Motor Nucleus of the vagus nerve (DMV). Thus, this hypothesis posits a sequential ladder of autonomic responses. Certainly, this sequence of autonomic reactions is not grounded in evidence: the functional distinctions made in polyvagal proposals ‒ between dorsal and ventral groups of neurons ‒ are unsupported by the scientific evidence and are often contradicted, as explained below.
PVT (e.g. Porges, 2007, 2011, 2023, 2024) relies upon an implausible claim about the functioning of the DMV: Via unmyelinated (slowly conducting) efferent fibers, the DMV is primarily responsible for mediating massive heart-rate decelerations (bradycardia) under various conditions, often related to emotionally traumatic events, and termed “dorsal vagal shutdown” (p. 179; and Porges, 2007, 2025b). The actual evidence and scientific consensus are, however, that the ventral vagal nucleus NA is predominantly involved in mediating both small and large heart-rate reactions (McAllen & Spyer, 1976; Geis & Wurster, 1980; Jones et al., 1995; Y. Wang et al., 2000; Jones, 2001; Cheng et al., 2002, 2004; Machhada et al., 2015, 2016, 2020; Farmer et al., 2016; Gourine et al., 2016; Ottaviani & Macefield, 2022: Veerakumar et al., 2022). The DMV has limited influence upon heart-rate control in mammals such as rats, cats, dogs and sheep, with numerous studies showing only modest effects. For example, a recent study with rats showed that strong stimulation of the DMV neurons using an optogenetic approach had no significant effect on heart rate (Kellet et al., 2024). Another recent mouse investigation demonstrated small DMV-mediated heart rate decelerations of 50 bpm (equal to or less than a 10% reduction in heart rate), related to activation of oxytocin receptor-positive DMV neurons (X. Wang et al., 2025).]
Grossman is not wrong. But he is not correct either. DMV neurons are contributory to salutogenic states. They do not specifically mediate lifethreat. They only lead to bradycardia under certain circumstances. In other states (safety) they function differently. The polyvagal cartography of state either does not understand this, or does not articulate it. It calls for substantive revision.
Autonomic neurology is variably recruited as a function of neuroception
Autonomic neurology collaboratively coordinates in the presence of signals of safety, and decoordinates in a patterned fashion in defense. This is mediated by neuroception and neurochemistry.
Shutdown in the body can be either systemic or localized
While there are full body shutdown states (what Polyvagal Theory calls dorsal vagal), shutdown can be highly localized in the body. Polvyagal Theory does not have an adequate explanatory framework for localization of shutdown.
Et cetera
These are some, but not all, of the major issues. My team has identified 39 issues in total.
FOUNDATION ERRORS IN NEUROSCIENCE
Many of the problems with PVT are problems with the field of neuroscience that predate the theory entirely and corrupt much of the research in the field
In creating PVT, Porges relied on neuroanatomical maps that preceded his work. This is an epistemological problem of validation, because the construction of validated scientific knowledge happens within an agreed upon framework that builds upon prior validated knowledge.
Nearly all of the extant neuro-anatomical maps of humans were made from cadavers. This means that they have at least two problems. First, when the body dies the finest ramifications of neurology degrade. This means that the neurology remaining was large enough not to degrade. This means that we are missing the level of detail at which neurology resolves into tissue, which is to say most of it. Second, anatomy is not the same as physiology, and neural impulses do not flow through dead bodies. Therefore it is nearly impossible to parse direction of flow which makes differentiating circuitry nearly impossible. I realize that there are novel in vivo techniques that get around this, but the inherited maps of the ANS are, at best, incomplete, and at worst extremely inaccurate. Mapping is furthermore siloed into discrete disciplinary areas. Furthermore, activation of neurology is mediated by neuroception. So the same neural systems function differently depending on a) neuroception, b) the presence or absence of specific neurochemistries.
This is both exciting and daunting on the research side, because identification of living neural firing is contingent on multiple contextual variables. This means you cannot simply put someone in an imaging circumstance, observe neural activity, and conclude that you have resolved a definitive pathway. These systems are hyper-complex.
Much of what Grossman fixates on, specifically RSA as the measurement tool, and how Porges came to his evolutionary conclusions, which are conjectural, can be revised without fundamentally undermining the primary insights of Polyvagal Theory.
This duly noted, our work in Autonomics extends and refines contentions of PVT, updating understanding of what autonomic state is, how it is constructed neurologically and neurochemically, and updating the functional mapping of the living ANS dramatically.
Instead of throwing the baby out with the bathwater, let’s raise the baby.
I have written an extremely detailed update of PVT in The Neurobiology of Connection, which is in narrative form, and much more fun to read than this article.
Thanks for your attention.
https://www.clinicalneuropsychiatry.org/download/when-a-critique-becomes-untenable-a-scholarly-response-to-grossman-et-al-s-evaluation-of-polyvagal-theory/
Thank you. Mic drop.
Well written, thank you!!