

TENABLE: RECONCILING POLYVAGAL THEORY WITH THE UTILITY OF THE GROSSMAN CRITIQUE
Raise baby, discard bathwater

This is not a fluff piece, and it is going to take you 15 or 20 minutes to read. I am an expert in applied autonomic physiology, the Founder of Hearth Science, the Developer of Autonomics, and the author of The Neurobiology of Connection. I had an intellectual property development agreement with Stephen Porges’ firm Polyvgal LLC for years. I wrote and art directed the Official Polyvagal Posters. If you want to understand what it is at stake in this debate, why it matters, and how the field could evolve, read on.
PART ONE: SETTING UP DISCOURSE PARAMETERS
BACKGROUND
For those of you who may not be privy to the re-ignition of the academic & mindshare battle between Polyvagal Theory and Paul Grossman, which has been simmering away for a couple of decades, Stephen W. Porges, PhD is the Developer of the Polyvagal Theory, which he proposed in 1994, as a systems level, pathway-specific framework of autonomic regulation.
The Autonomic Nervous System (ANS) is the neural architecture of the mindbody connection: it controls the deepest and most powerful levers that govern your moment-to-moment experience of wellbeing. While most people who know that the ANS exists understand that it regulates the internal milieu of the body, adjusting breathing, heart-rate, digestion, and other internal bodily functions (automatically) in response to moment-to-moment inner and outer contextual changes in our environment, the general population does not recognize the role that the ANS plays in selectively re-tuning the body and mind based on whether we find ourselves to be safe or in danger.
This is to say that the ANS governs both our relaxation and stress responses. It is, functionally, the deepest strata of the human operating system. It is the extra-cranial embodied brain. The neurology of your oceanic bodily intelligence. It shapes the biological/ neurological glasses that color your view of the world in each and every moment.

Since 80% of what brings people into primary care settings is stress-related1, understanding HOW and WHY the ANS does this is of paramount importance to the study of human well and illbeing. Porges’ work represents a significant breakthrough, both in its implications and applications, refining the scope of this understanding. Its uptake into trauma therapy, somatics, mindful awareness and other domains of wellness has been, therefore, remarkable and merited.
Porges is a psychologist with multiple university appointments who was past president of the Society for Psychophysiological Research and the Federation of Associations in Behavioral & Brain Sciences. He is a former recipient of a National Institute of Mental Health Research Scientist Development Award. He has published more than 400 peer-reviewed papers across numerous disciplines including anesthesiology, neurology, neuroscience, pediatrics, psychiatry, psychology, and psychometrics. He holds multiple patents for developing psychophysiology methods and systems.
Polyvagal Theory is a significant trans-disciplinary synthesis. It draws from a wide range of academic disciplines, and was assembled both as a result of Steve’s direct experience2, and his attempts to resolve the ‘vagal paradox’3. It is, in my humble opinion, the most significant update to the ANS of the second half of the 20th century, and I believe that Porges should receive the Nobel Prize in Physiology or Medicine for this work. But, here’s the thing– I worked closely with Steve from 2019-2021, specifically focused on translating his work for the general population, and applying it in clinical contexts– and Polyvagal Theory IS incomplete.
Steve knows this. People who are deeply familiar with the theory know this. It is not, in fact, a secret amongst people who have rigorously studied the theory beyond the simplifications presented in the general public discourse.

THE ARGUMENT
In the latest issue of Clinical Neuropsychiatry, Paul Grossman, who is Emeritus Research Director in Psychosomatic Medicine at University Hospital Basel, is the lead author of an article entitled WHY THE POLYVAGAL THEORY IS UNTENABLE, which has 38 co-authors with expertise in the Vagus, which has been blowing up the internet. Porges, for his part, has written a rebuttal of the critique in the same issue, When a Critique Becomes Untenable: A Scholarly Response to Grossman et al.’s Evaluation of Polyvagal Theory.
My LinkedIn feed, since then, has filled with this kind of tripe:

So rapid is the internet’s uptake of this bullshit that the final article, which was written by someone whose byline is just ‘Ana’ - no last name- is that even a person? is being cited by Google’s Gemini search engine AI as part of the evidence PVT has been found untenable, which is how I found the article in the first place. Which is to say plainly that a critique that is itself limited in scope and utility is now being echoed by pundits and fed into blackbox AI, where it is becoming part of the fact set undergirding the discourse parameters of this conversation. Alarming.
THE BIGGEST PROBLEM WITH THIS: ALL OF US LOSE
The biggest problem with all of this? The Grossman paper is USEFUL. It is important. And in a world where we could distinguish signal from noise, where there was more humility and less saber-rattling, this could and should be the catalyst we need to continue to refine Polyvagal Theory, which needs to be refined!
Instead, we get Porges and Grossman talking past one another, Grossman in AN ALL CAPS JOURNAL ARTICLE, and Porges refusing to engage the terms of Grossman’s critique. While I can understand both of their positions– Grossman’s indignation, and Porges’ refusal to engage (the history of this debate is laid out by the Polvyagal Institute here), and they are not wrong about it– this is creating a situation where both sides fail to engage the meaningful opportunity to advance our understanding of the autonomic nervous system: the biological system that regulates the deepest and most powerful levers that govern our moment-to-moment experience of wellbeing. The churn being created for those in healthcare and mental health, and those served by them, rather than being productive to scientific discourse, is generating fear, confusion, disorientation, and shitty sensationalist articles that amplify fear, confusion, and disorientation. Although I understand Porges’ objection to the discourse terms, and his sense that a straw man of the theory is being attacked, the problem is that now this is being adjudicated in the court of public opinion, where it is being decided by people with the least likelihood of understanding the nuances involved, and where the people who SHOUT THE LOUDEST are drowning out calmer and demonstrably more informed voices. That is the wherefore of this particular article.
Instead of trying to decide who won the argument, let’s evolve the conversation. Let us therefore set down the two men, and simply engage their ideas.
PART TWO: TOWARDS TENABILITY
With an explicit objective to get Porges and Grossman’s ideas (and not persons) into conversation with one another, I offer the following assertions, which I believe will be palatable to both, having closely read and reviewed Grossman’s paper regarding PVT’s UNTENABILITY and Porges’ scholarly response.
Steve, Paul- you are both going to see this article- let me know if I have said something you cannot accept. I’m sure Paul will- he’s not the quiet type ;)
WHAT CAN WE ALL AGREE THAT POLYVAGAL THEORY HAS GOTTEN RIGHT?
There are three Autonomic Systems
Stephen Porges’ recognition that the 10th cranial nerve, the Vagus, is not a single nerve, but rather a conduit that holds multiple vagal systems (one supra-diaphragmatic, one sub-diaphragmatic)(one significantly myelinated, the other less so), subtending distinct visceral systems, with distinct physiological pathways, and differentially involved in responses to safety, danger, and lifethreat is THE MAJOR AUTONOMIC DISCOVERY of the second half of the 20th century, and for which Porges should receive the Nobel Prize in Physiology or Medicine. It is that important.
This updates the still-taught-in-medical-school-though-it-is-a-hundred-years-out-of-date notion of autonomic balance between the ‘parasympathetic’ and ‘sympathetic’ branches of the ANS. Autonomic balance is demonstrably false, yet almost everyone in the world who knows anything about the ANS as a mediator of stress responses believes that this is how it works.
Autonomic balance is built into medical models, and underpins the algorithms running the HRV sensors in your smart watch.
The vagal experts and Porges can agree: there are three autonomic systems, two of which are vagal. Paul Grossman doesn’t like to admit this, but here’s the problem. They are fundamentally unable to refute it.4 This is extremely important.
Interoception as ontological
Porges orients us towards interoceptive awareness as a metric of being. He suggests that rather than an identity resident in thinking, interoception is the location of our experience of embodied self, and where we might find ourselves at home.
It is not, as Descartes would have it, I think therefore I am. It is I feel (myself), therefore I am.
Variable recruitment of autonomic systems across the range of safety, danger, and lifethreat
Porges proposes a neurological mechanism (he coined the term neuroception) for the body’s moment-to-moment detection of safety, danger, or lifethreat.
Depending on whether the body feels safe enough to become available relationally (social engagement) or rather moves into states of defense (fight-flight, shutdown, etc.) the three autonomic systems engage differentially.
The three autonomic neurologies are differentially available depending on whether someone is experiencing safety, danger, or lifethreat.
This matters broadly because people’s autonomic nervous system is recalibrating moment-to-moment based on whether we feel safe, in danger, or under lifethreat. For most people, this is happening entirely outside of conscious awareness. If people understood this, and had interoceptive access to what it means (if they could FEEL it), we would live very different (and better) lives.
Porges understands this phenomenon of autonomic state as an intervening variable between physiology and behavior.
“At its core, Polyvagal Theory proposes that autonomic state functions as an intervening variable ‒ a neurophysiological platform that shapes how organisms detect, evaluate, and respond to cues of safety, danger, and life threat (Porges, 2007b, 2023).”5

The human nervous system comes with physiological presets (autonomic states), somewhat like the tuning presets on a stereo. These energy-processing templates modulate our physiology to filter our experience.
When I feel safe enough to become relationally available to others, my physiology moves into synchrony, and is functioning in a way that is totally different (and health-creating), while when I shift into defensive responses to danger my physiology functions differently. If I cannot shift out of these defensive states, they are pathogenic (disease-creating). In other words, if a stress response becomes chronic and non-resolving, I am going to become ill.
Safety is a pre-condition of sociality, which is a precondition for wellbeing.
We talk about disparities in access to housing, food, money, etc., but our public health discourse does not penetrate to the strata beneath this, which is the inequitable distribution of safety. When people feel safe enough in their bodies, they have access to different visceral states, emotions, cognitions, perceptions of the world around them, and different behaviors. They develop a different existential sense of self. The foundational substate of this experience is physiological, not psychological.
For the past 12,000 years, humans have been moving away from our species normal ancestral baseline in safety and connection, into states of physiological defense. Modernity is, in a way, the aggregate activity of humans who have moved into chronic states of defense. We are therefore generating culture and civilization from the perspective of traumatized and neurobiologically dysfunctional humans, who have been acculturated to think this is species normal. It is not. We call these things human nature, but they are the products of a traumatized human nature: people whose bodies are accustomed to operating in response to chronic danger and do not know this. We need safety to come home to ourselves. Polyvagal Theory taught the world this in the language of neurophysiology.
Human wellbeing is social in nature
The evolutionary species’ normal of the human lineage is the small band hunter gatherer group. Human wellbeing is social in nature. What Porges calls the ‘ventral vagal’ system (myelinated supra-diaphragmatic vagus), which undergirds the ‘social engagement complex’ that unites the neural regulation of the face, voice, tuning of the middle ear, turning of the neck and head, with the heart and the lungs, is the neurophysiological system whose availability is required as the prelude to secure attachment. (The Porgesian conceptualization of this system is, however, incomplete.)
States of chronic defense are incompatible with wellbeing and become a primary substrate for illbeing
The movement into chronic states of defense, which decouples the ventral vagal system from the other two autonomic systems, prevents the body from coordinating states of health, growth, and restoration. Sustained shifts into defense provide a primary physiological substrate of most classes of illbeing. When autonomic physiology is centralized as the diagnostic axis of disease etiology, it transforms our understanding of the mechanisms of much disease.
WHAT IS USEFUL IN GROSSMAN’S CRITIQUE?
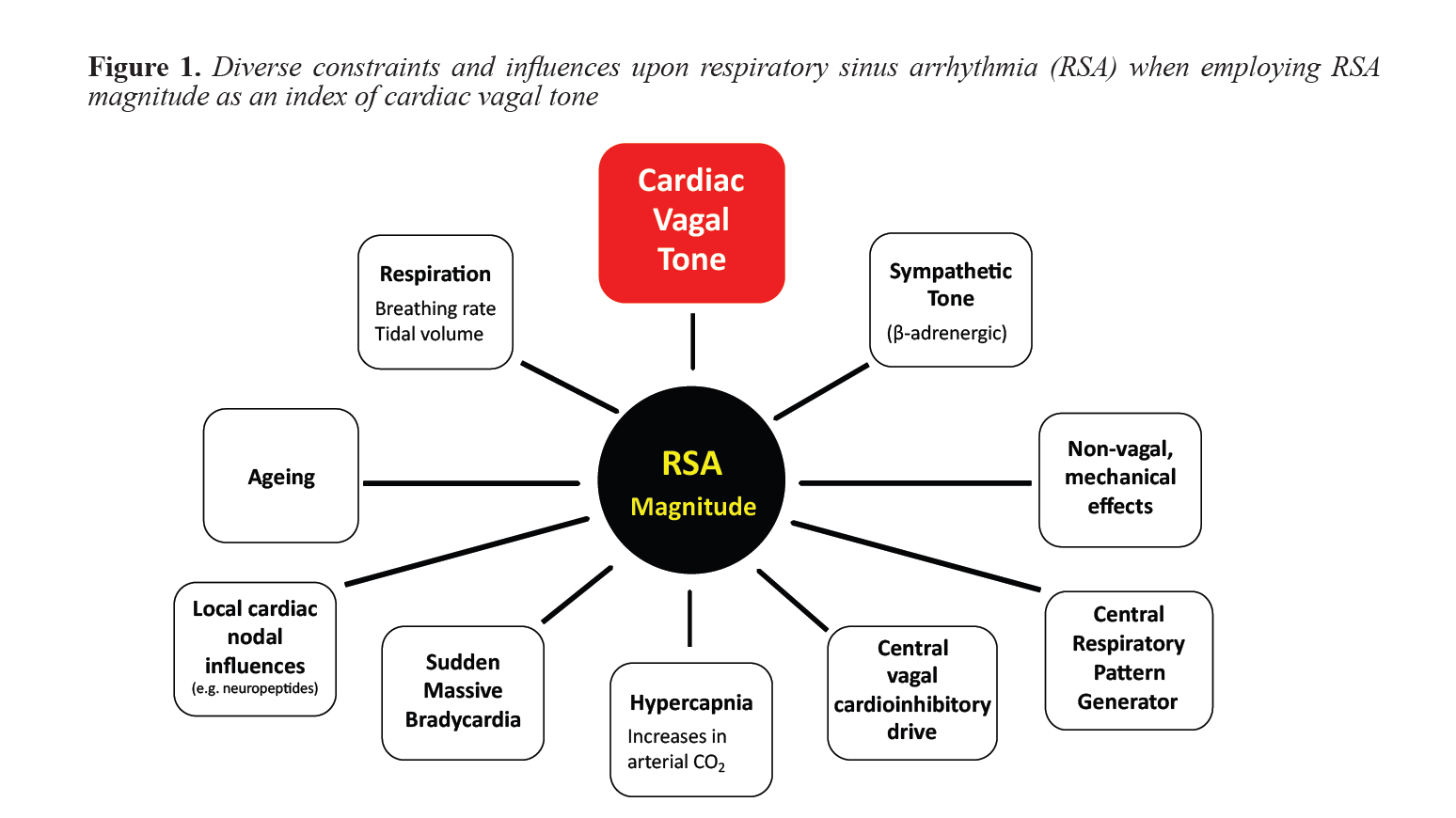
RSA is not the most complete autonomic signal
The first part of the Grossman critique is that Respiratory sinus arrhythmia is not a direct and reliable measure of central vagal outflow to the heart (mediated by the ventrally located brainstem Nucleus Ambiguus)
This is true. Its implications also extend far beyond Polvyagal Theory. If RSA is not a direct and reliable measure of central vagal outflow, every heart-rate variability monitor in the world is wrong, including the one you are wearing on your wrist. Your wearables are wrong. Your health-tracking ring is wrong, et cetera.6
Although RSA/HRV (Heartrate Variability) metrics have become the de facto standard for autonomic measurement, this is not due to the intrinsic superiority of HRV as an autonomic signal, but rather largely due to historical factors related to its measurability and the available compute in the 1960s when psychophysiology techniques were initially developed and deployed to measure autonomic phenomena in vivo.
Respiration is a more complete autonomic signal. I would propose that Stephen Porges would have developed a very different articulation of Polyvagal Theory had he been looking at the realtime functioning of the ANS through the lens of respiration, rather than cardiac control.
What is the opportunity here?
Let’s utilize respiration as the primary autonomic signal to test the assertions of Polyvagal Theory. Rather than simply condemning RSA, let’s test using a better autonomic measurement technology. Here is a paper about a non-invasive physiological measure that uses respiration as the primary signal that actually works.
If RSA is the problem, let’s test the Polyvagal hypotheses using a different autonomic diagnostic technology. I have a recommendation if you are a researcher and would care to know.
The Autonomic Nervous System is not a ladder
I have been writing about this for years. Despite the fact that Polvyagal Institute teaches the ANS as a hierarchy, with ventral at the top, and dorsal at the bottom, and frames this understanding by way of reference to Jacksonian Dissolution, which is the notion that in dealing with a threat we recruit the evolutionarily newest autonomic systems until they fail, and then fall back to the next oldest systems, this is not how the ANS constructs autonomic state. Grossman justly critiques this framing by explaining that the functional differentiation between neurology in the brainstem NA and DMX do not map as cleanly along the lines of differentiation as PVT would suggest.
Polyvagal Conceptualization of state is inadequate
The Polvyagal conceptualization of autonomic state, its notion of which autonomic states exist, and their conceptual arrangement is not accurate or complete. Humans routinely flow in and out of autonomic states that are not on the Polyvagal map, and the composition of health-creating states is not correct. The notion of hybrid states is incomplete. The ‘sympathetic’ nervous system is regularly recruited without danger. Variable neurochemistries of connection, activation, and shutdown create polyphonic modes of autonomic states with degrees of nuance. The subdiaphragmatic vagus (PVT - dorsal vagus) is actually recruited in states where we have the neuroception of safety.
[The Polyvagal arguments about functional differentiation between NA/ DMX are refuted directly by Grossman here:
GROSSMAN: Specious functional distinctions between vagal dorsal (Dorsal Motor Nucleus) and ventral (Nucleus Ambiguus) regions of the brainstem
Primary to PVT is the idea that human behavioral functioning to aversive and appetitive psychosocial stimuli depends upon a hierarchy of autonomic responses: First, calm and prosocial behavior is said to be parasympathetically mediated by the brainstem “ventral vagal complex” (most directly, the Nucleus Ambiguus [NA]). Second, PVT asserts that individuals experiencing severe stress mount sympathetic nervous system reactions of fight or flight. Third, in very dire or life-threatening circumstance, a defensive pattern of emotional freezing or psychological dissociation may occur, which is parasympathetically mediated by the Dorsal Motor Nucleus of the vagus nerve (DMV). Thus, this hypothesis posits a sequential ladder of autonomic responses. Certainly, this sequence of autonomic reactions is not grounded in evidence: the functional distinctions made in polyvagal proposals ‒ between dorsal and ventral groups of neurons ‒ are unsupported by the scientific evidence and are often contradicted, as explained below.
PVT (e.g. Porges, 2007, 2011, 2023, 2024) relies upon an implausible claim about the functioning of the DMV: Via unmyelinated (slowly conducting) efferent fibers, the DMV is primarily responsible for mediating massive heart-rate decelerations (bradycardia) under various conditions, often related to emotionally traumatic events, and termed “dorsal vagal shutdown” (p. 179; and Porges, 2007, 2025b). The actual evidence and scientific consensus are, however, that the ventral vagal nucleus NA is predominantly involved in mediating both small and large heart-rate reactions (McAllen & Spyer, 1976; Geis & Wurster, 1980; Jones et al., 1995; Y. Wang et al., 2000; Jones, 2001; Cheng et al., 2002, 2004; Machhada et al., 2015, 2016, 2020; Farmer et al., 2016; Gourine et al., 2016; Ottaviani & Macefield, 2022: Veerakumar et al., 2022). The DMV has limited influence upon heart-rate control in mammals such as rats, cats, dogs and sheep, with numerous studies showing only modest effects. For example, a recent study with rats showed that strong stimulation of the DMV neurons using an optogenetic approach had no significant effect on heart rate (Kellet et al., 2024). Another recent mouse investigation demonstrated small DMV-mediated heart rate decelerations of 50 bpm (equal to or less than a 10% reduction in heart rate), related to activation of oxytocin receptor-positive DMV neurons (X. Wang et al., 2025).]
Grossman is not wrong. But he is not correct either. DMV neurons are contributory to salutogenic states. They do not specifically mediate lifethreat. They only lead to bradycardia under certain circumstances. In other states (safety) they function differently. The polyvagal cartography of state either does not understand this, or does not articulate it. It calls for substantive revision.
GOING FURTHER THAN GROSSMAN
Polyvagal Theory is demonstrably incomplete. I worked closely with Steve for several years, and he knows this. There are two categories of errors in the theory, namely (1) errors in the foundation of modern neuroscience & (2) errors in the PVT conceptualization…
ERRORS IN THE FOUNDATION OF MODERN NEUROSCIENCE
Errors in the foundation of modern neuroscience result from necrotic anatomy, failure to differentiate neuro-anatomy from neurophysiology, and errors as a result of the brain-centric bias of the field entire. This means that many of the neuro-anatomical maps, and autonomic neuro-taxonomies Porges inherited were wrong. It means that the functional differentiation of primary autonomic systems is not accurate.
There is, for example, no such thing as the Sympathetic Nervous System. What we call the Sympathetic Nervous System is the vertebrate Movement System under specific contextual conditions where its neurochemistry is preferentially driven by adrenaline and cortisol. The notion of the system being ‘sympathetic’ conjoins neurology and neurochemistry that can function independently. e.g., there are autonomic states where this neurology functions with other neurochemistries. If this neurology is utilized in autonomic states outside of fight-or-flight (as it does when we are playing, competing, etc.), the extant neurotaxonomic framework is demonstrably obsolete. In as much as PVT is wrong in these and other particulars, as a result of inheriting faulty maps, so are nearly all extant neuro-anatomical and neurophysiological models.
ERRORS IN PVT SPECIFICALLY
Porges states (section 2.5) Polyvagal Theory: Conceptual Clarification: Polyvagal Theory is explicitly formulated as a testable neurophysiological framework. Its core propositions generate falsifiable predictions regarding the organization of brainstem autonomic circuits, the functional role of autonomic state as an intervening variable, and the conditions under which social engagement, defensive mobilization, or metabolic conservation are expressed. Among these core predictions, the theory would be empirically challenged if ventral vagal (NAmb-originating) activity were shown to increase during conditions of life threat or defensive immobilization rather than being withdrawn as predicted by hierarchical state regulation; if robust social engagement reliably occurred in the absence of ventral vagal regulation or during dominance of dorsal vagal or sympathetic circuits; if developmental maturation of NAmb myelination failed to correspond with the emergence of RSA, vagal efficiency, and social regulatory capacities; or if central coordination of respiratory and cardioinhibitory activity were shown to be epiphenomenal rather than reflecting an integrated regulatory network.
There is an additional category of falsifiability that would directly lead to empirical challenge, namely the presence of ‘dorsal vagal’ activity during ventral vagal activities. Part of Grossman’s paper has addressed the mechanism of such a challenge. Our work has measured this autonomically using respiration as the primary autonomic signal. This directly challenges the current PVT construction of the ‘autonomic ladder’.
This is to say that the sub-diaphragmatic vagal system (what Porges calls dorsal vagal) is also involved in salutogenic states. Its neural architecture supports states of health, growth, and restoration: it does not merely undergird states of lifethreat. The PVT hierarchy of state, and conceptual construction of state is not accurate.
PART THREE: IN CONCLUSION
PVT is a trans-disciplinary synthesis, and some of its particulars need refinement, yet this does not undermine the foundational nature of its insights. Instead of throwing the baby out with the bathwater, let’s raise the baby. I have written an extremely detailed update of PVT in The Neurobiology of Connection, which is in narrative form, and much more fun to read than this article.
Imagine what might happen if there was a productive dialog around the actual science between people who actually understood PVT in a profound way, and Grossman’s 39 scientist colleagues expert in the Vagus. If we could harness the collective intelligence of such an extraordinary group towards the common goal of better understanding the profound beauty and mystery of these systems that are so central to human well and ill-being (and what the fuck else would be a better use of their time?) imagine the advancements that could be made.
Yet in order to do this, we would need a climate of some degree of relational safety and respect, such that opening into relational availability to one another, we did not risk being harmed by the harsh words, shouts, and strident attacks of one another. If I were going to sit down with Paul Grossman and share what I understand– what I have learned through several decades of profound study and profound sacrifice– I would need to feel that he was balanced enough not to attack me– otherwise, why would I bother? Instead, I would simply seal the deepest, truest, most brilliant parts of myself off in some other form of defense, actively through confrontation or escape, or perhaps move into a deeper shutdown where I was immobilized by the shame of being attacked so publicly by such an esteemed global expert. Maybe, if I was afraid he was more powerful than me, I would move into some form of appeasement, and if I was really overwhelmed, I might try to placate him.
In order to actually reach new ground, to actually uncover something beyond what either of us know, we would have to lower our defenses enough to be open. And in a world filled with uncertainty, that feels Brittle, Anxious, Non-Linear and Incomprehensible, this is very hard to do. It is much easier to retreat, tribally, with those who agree with me, and SHOUT ACROSS THE CHASM. Or simply fail to engage.
Thankfully, there is a neurophysiological framework, a sort of lens, that can help us conceptualize the guardrails that would be required to create the conditions where we might be together and down-regulate our defensive responses. The first incarnation of this framework is called Polyvagal Theory. Thank goodness such a framework exists. Let’s get to version 2.0.
There are number of places where this figure is used, including here.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4286362/
See my 2021 interview with Stephen W. Porges, PhD, as part of the Connection Masterclass, where he speaks about learning to play the clarinet as a vagal exercise.
Porges writes about publishing a paper in a journal of Neonatology, talking about the protective power of the vagus. He received a letter from a neonatologist who thanked him for the paper, but said that he had learned in medical school that the vagus could kill an infant. How, Porges wondered, could the same nerve be both protective and the source of life-threatening bradycardia (sudden drop in heart rate?). This paradox led him to structure the question that would resolve in the formation of the Polyvagal Theory in 1994.
From https://www.polyvagalinstitute.org/criticaldiscussionofpolyvagaltheory
“In addition to peer-reviewed publications, public-facing sources—particularly the Wikipedia entry on Polyvagal Theory—have played a role in disseminating inaccuracies. That entry prominently cites two critiques: Neuhuber and Berthoud (2022) and Doody, Burghardt, and Dinets (2023). While both articles were peer-reviewed, their appearance in a special issue of Biological Psychology edited by Grossman suggests an editorial alignment that likely shaped both their thematic and conceptual framing.
The critique by Neuhuber and Berthoud exemplifies an anatomical-functional misinterpretation. While questioning the functional interpretation of vagal pathways proposed by Polyvagal Theory, they do not dispute the core neuroanatomical distinctions—specifically, the separation between the dorsal motor nucleus of the vagus (DMNX) and the nucleus ambiguus (NAmb), nor the contrasting myelination of their efferents. However, they omit a critical tenet of the theory: that the Social Engagement System (SES) derives from structures of the embryological pharyngeal arches and that communication between the cardioinhibitory vagus and the SES is largely indirect, with the exception of direct pathways involving the trigeminal nerve. Wikipedia, in summarizing this critique, distorts it further—presenting it as a categorical refutation of the anatomical foundation of Polyvagal Theory, which the original article does not claim.”
https://www.clinicalneuropsychiatry.org/download/when-a-critique-becomes-untenable-a-scholarly-response-to-grossman-et-al-s-evaluation-of-polyvagal-theory
Section 2.1
https://www.researchgate.net/publication/396679935_AUTONOMIC_DIAGNOSTICS_Towards_Accurate_In_Vivo_Autonomic_Measurement
May there be enough curiosity (a function of being safe enough) to move this exploration forward. Such important work. Thanks for your contribution here Gabriel.
Hear hear!